CNN journalist admits that US diplomats were hit with v2k acoustic torture attacks in Cuba, including voices and messages
—————————————————————————————————————————————————————————
Column: Are electromagnetic weapons involved? Taking victims of ‘Havana syndrome’ seriously
BY Jean Guerrero
Posted on https://www.latimes.com
on February 24, 2022
The U.S. investigation into mysterious symptoms known as the “Havana syndrome” could provide Americans with long-overdue insights into the emerging threats of directed-energy devices.
Hundreds of U.S. government personnel — mostly spies and diplomats abroad — have reported piercing pain, unexplained sounds, vertigo, vision loss, memory loss, insomnia and signs of brain damage since 2016, when dozens were afflicted in Cuba.
Later incidents were reported in China, Russia, Colombia, Austria, Uzbekistan, the United Kingdom, Poland and other countries. While some theories blamed mass hysteria and even crickets, a rise in high-profile cases — including in and around the White House — compelled U.S. officials to seriously consider a more nefarious and disturbing explanation: unseen electromagnetic weapons.
The official term for this syndrome is “anomalous health incidents.” A State Department spokesperson told me that “to date, no study, report or analysis has provided a categorical, comprehensive explanation.”
Earlier this month, a Biden administration expert panel rejected the idea that “psychosocial factors alone” explained symptoms. “Pulsed electromagnetic energy, particularly in the radiofrequency range, plausibly explains the core characteristics, although information gaps exist,” it stated. Its report reaffirmed a 2020 National Academies of Sciences, Engineering, and Medicine theory citing “directed, pulsed radio frequency (RF) energy.”
In October, President Biden signed into law the bipartisan “Helping American Victims Afflicted by Neurological Attacks Act,” to provide care and compensation to government employees with symptoms. An official with the House Intelligence Committee chaired by Rep. Adam B. Schiff (D-Burbank) told me the committee is “closely overseeing implementation of the HAVANA Act to ensure that all personnel receive the benefits and assistance they need.” It may sound like science fiction, like the military’s UFO probe. But it wouldn’t be the first time U.S. personnel were zapped by electromagnetic weapons. Between the 1950s and 1970s, the Soviets bombarded the U.S. Embassy in Moscow with microwave radiation, prompting health concerns and this country’s then-classified exploration of such weaponry.
After the Cold War, debates about the technology’s dangers became the near-exclusive realm of people ridiculed as tin-hat conspiracy theorists. In 2001, then-Rep. Dennis Kucinich (D-Ohio) introduced legislation to ban the weaponization of “radiation, electromagnetic” or other energies against people, but it was dropped following media derision. Meanwhile, the U.S. military continued developing such weapons, including the Active Denial System, or “Pain Ray.”
The U.S. has been slow to respond to reported attacks against government personnel that many attribute to Russia. In January, a CIA report dismissed all but a couple dozen reports as having mundane explanations such as stress. But in a CBS “60 Minutes” report, “Targeting Americans,” which aired Sunday, CIA Director William Burns, whose colleague reported symptoms in India last fall, said he was taking reports seriously.
Watching this documentary, I thought about the thousands of private citizens who call themselves “targeted individuals” who’ve reported similar experiences, including perceived attacks by remote-controlled weapons causing long-term illness. They have been sounding the alarm for years about possible electromagnetic weaponry deployment on U.S. soil, but they’ve been derided as delusional. Among them is my father.
A Mexican immigrant who worked in shipbuilding in San Diego before he was laid off, he believes the CIA experimented on him with electromagnetic weapons that caused him to collapse in pain and develop insomnia, among other things.
In his telling, which he’s never been able to prove, the CIA was testing the weapons’ ability to dramatically alter behavior — by targeting drug addicts with electronic intervention. (My father was using crack cocaine, and quit because of this perceived intervention.) Since telling his story in my memoir, I’ve received dozens of emails from others who claim they’re victims of similar electronic torture.
Investigations into the cause or causes of the “Havana syndrome” could offer some answers for these people, too. Of course, many are deeply skeptical of the CIA’s ability to uncover the truth given its history of secret psychological torture experiments targeting marginalized people starting in the 1950s.
The White House has not said whether the investigation would include cases involving private citizens. The victims’ legislation applies only to government personnel and their families. But Miles Taylor, a former Department of Homeland Security chief of staff in the Trump administration — who revealed his personal experiences of “Havana syndrome” symptoms in the “60 Minutes” report — told me he believes some testimony from private citizens is worthy of investigation, too.
“Authoritarian nation-states will go after their enemies regardless of whether they wear a government badge or not,” he said. “If these attacks are indeed being perpetrated by a nation like Russia, it wouldn’t surprise me if private citizens in certain capacities would be targeted for reasons that would advance the Kremlin’s agenda.”
Taylor hopes his “60 Minutes” testimony will encourage other victims to report. Many stay silent for fear of being perceived as mentally unstable. Since the report aired, he’s been contacted by multiple intelligence leaders and others with similar experiences. “I think we’ve only seen the tip of the iceberg,” he told me.
The investigation includes the State Department, the CIA and the departments of Homeland Security, Defense and Justice. They have until Friday to update their guidance for personnel. Earlier this month, Biden named the National Security Council’s senior director for intelligence programs, Maher Bitar, as interagency coordinator. But it’s not enough.
Mark Zaid, an attorney who has represented numerous government victims dating back to the 1990s, criticized the response as “completely disorganized and non-uniform.”
Zaid worries the legislation will be implemented unfairly, leaving people out. Olivia Troye, former Vice President Mike Pence’s homeland security and counterterrorism advisor — who also spoke to “60 Minutes” about her experience with the syndrome — shared similar concerns with me.
The Biden administration should create a centralized location for reporting cases, including by private citizens. The U.S. can’t appropriately compensate victims without understanding the syndrome’s causes. That’s why investigators should scrutinize the United States’ own potential abuse of such technology, and collect testimony outside of U.S. government personnel. Private citizens who’ve been reporting similar attacks since at least the early 2000s deserve to be heard.
Most of their claims may be baseless. But the health problems reported by high-ranking officials with no history of mental illness offer evidence that we should not categorically dismiss them.
—————————————————————————————————————————————————————————
Havana syndrome and targeted individuals
—————————————————————————————————————————————————————————
Experts Believe US Embassies Were Hit With High-Power Microwaves – Here’s How the Weapons Work
By Edl Schamiloglu
Posted on https://www.scitechdaily.com
on February 12, 2022
{kind=link}

Some of the cases of the mystery ailment that has afflicted U.S. embassy staff and CIA officers off and on since 2016 in Cuba, China, Russia, and other countries most likely were caused by pulsed electromagnetic energy, according to a report by a panel of experts convened by national intelligence agencies.
The report’s findings are similar to those of another report released by the National Academies in 2020. In that report, a committee of 19 experts in medicine and other fields concluded that directed, pulsed radiofrequency energy is the “most plausible mechanism” to explain the illness, dubbed “Havana syndrome.”
Neither report is definitive, and their authors don’t address who targeted the embassies or why they were targeted. But the technology behind the suspected weapons is well understood and dates back to the Cold War arms race between the U.S. and the Soviet Union. High-power microwave weapons are generally designed to disable electronic equipment. But as the Havana syndrome reports show, these pulses of energy can harm people, as well.
As an electrical and computer engineer who designs and builds sources of high-power microwaves, I have spent decades studying the physics of these sources, including work with the U.S. Department of Defense. Directed energy microwave weapons convert energy from a power source – a wall plug in a lab or the engine on a military vehicle – into radiated electromagnetic energy and focus it on a target. The directed high-power microwaves damage equipment, particularly electronics, without killing nearby people.
Two good examples are Boeing’s Counter-electronics High-powered Microwave Advanced Missile Project (CHAMP), which is a high-power microwave source mounted in a missile, and Tactical High-power Operational Responder (THOR), which was recently developed by the Air Force Research Laboratory to knock out swarms of drones.
https://www.youtube.com/embed/Ogi_o8dszrk?feature=oembed
A news report about the U.S. Air Force’s high-power microwave anti-drone weapon THOR.
Cold War origins
These types of directed energy microwave devices came on the scene in the late 1960s in the U.S. and the Soviet Union. They were enabled by the development of pulsed power in the 1960s. Pulsed power generates short electrical pulses that have very high electrical power, meaning both high voltage – up to a few megavolts – and large electrical currents – tens of kiloamps. That’s more voltage than the highest-voltage long-distance power transmission lines, and about the amount of current in a lightning bolt.
Plasma physicists at the time realized that if you could generate, for example, a 1-megavolt electron beam with 10-kiloamp current, the result would be a beam power of 10 billion watts, or gigawatts. Converting 10% of that beam power into microwaves using standard microwave tube technology that dates back to the 1940s generates 1 gigawatt of microwaves. For comparison, the output power of today’s typical microwave ovens is around a thousand watts – a million times smaller.

{kind=link}
The development of this technology led to a subset of the U.S.-Soviet arms race – a microwave power derby. When the Soviet Union collapsed in 1991, I and other American scientists gained access to Russian pulsed power accelerators, like the SINUS-6 that is still working in my lab. I had a fruitful decade of collaboration with my Russian colleagues, which swiftly ended following Vladimir Putin’s rise to power.
Today, research in high-power microwaves continues in the U.S. and Russia but has exploded in China. I have visited labs in Russia since 1991 and labs in China since 2006, and the investment being made by China dwarfs activity in the U.S. and Russia. Dozens of countries now have active high-power microwave research programs.
Lots of power, little heat
Although these high-power microwave sources generate very high power levels, they tend to generate repeated short pulses. For example, the SINUS-6 in my lab produces an output pulse on the order of 10 nanoseconds, or billionths of a second. So even when generating 1 gigawatt of output power, a 10-nanosecond pulse has an energy content of only 10 joules. To put this in perspective, the average microwave oven in one second generates 1 kilojoule, or thousand joules of energy. It typically takes about 4 minutes to boil a cup of water, which corresponds to 240 kilojoules of energy.
This is why microwaves generated by these high-power microwave weapons don’t generate noticeable amounts of heat, let alone cause people to explode like baked potatoes in microwave ovens.
High power is important in these weapons because generating very high instantaneous power yields very high instantaneous electric fields, which scale as the square root of the power. It is these high electric fields that can disrupt electronics, which is why the Department of Defense is interested in these devices.
How it affects people
The National Academies report links high-power microwaves to impacts on people through the Frey effect. The human head acts as a receiving antenna for microwaves in the low gigahertz frequency range. Pulses of microwaves in these frequencies can cause people to hear sounds, which is one of the symptoms reported by the affected U.S. personnel. Other symptoms Havana syndrome sufferers have reported include headaches, nausea, hearing loss, lightheadedness and cognitive issues.
The report notes that electronic devices were not disrupted during the attacks, suggesting that the power levels needed for the Frey effect are lower than would be required for an attack on electronics. This would be consistent with a high-power microwave weapon located at some distance from the targets. Power decreases dramatically with distance through the inverse square law, which means one of these devices could produce a power level at the target that would be too low to affect electronics but that could induce the Frey effect.
The Russians and the Chinese certainly possess the capabilities of fielding high-power microwave sources like the ones that appear to have been used in Cuba and China. The truth of what actually happened to U.S. personnel in Cuba and China – and why – might remain a mystery, but the technology most likely involved comes from textbook physics, and the military powers of the world continue to develop and deploy it
Written by Edl Schamiloglu, Distinguished Professor of Electrical and Computer Engineering, University of New Mexico.
—————————————————————————————————————————————————————————
External energy source may explain ‘Havana syndrome,’ panel finds, renewing questions about possible foreign attack
By Shane Harris
Posted on https://www.washingtonpost.com
on February 2, 2022
The finding by experts convened by U.S. intelligence agencies suggests that a foreign power could have mounted attacks on U.S. diplomats, intelligence officers and military personnel serving overseas
An external energy source may explain disorienting and sometimes debilitating symptoms suffered by U.S. government personnel, a panel of experts has found, reaching a conclusion that, while not definitive, suggests a foreign power could have mounted attacks on U.S. diplomats, intelligence officers and military personnel serving overseas.
The findings by the expert panel, which was convened by U.S. intelligence agencies, are the latest attempt to solve the years-long mystery of what, or who, is behind a constellation of symptoms known as “Havana syndrome.” In late 2016, personnel at the U.S. Embassy in Cuba’s capital reported a range of sensations including ringing and pressure in the ears, headaches and dizziness. Personnel in China later experienced similar symptoms, which have now been reported by hundreds of people serving at official posts around the world.
The vast majority of those cases have been attributed to medical conditions or other environmental factors, officials have said.
An earlier interim report from the CIA found that a foreign country is probably not mounting a global attack aimed at U.S. personnel. People who say they are victims of Havana syndrome strongly criticized the agency’s findings.
But the CIA report didn’t expressly rule out a foreign hand, at least behind some small number of cases for which investigators have found no cause or plausible explanation.
The expert panel’s finding was consistent with earlier conclusions from the National Academies of Sciences, Engineering and Medicine, which found that “directed, pulsed radio frequency energy appears to be the most plausible mechanism in explaining these cases.”
That study was chaired by David Relman, a professor of microbiology and immunology at Stanford University, who also worked with the intelligence community’s panel of experts. The panel did not attribute any cases to a specific device or country.
The experts included people from within and outside the U.S. government, with expertise in science, medicine and engineering. They were given access to classified government information on reported incidents and trends, and met with individuals who shared their personal experiences and medical records, according to intelligence officials familiar with the panel’s work, who spoke on the condition of anonymity under ground rules established by the intelligence agencies.
As a starting point, the panel examined “the plausibility of five potential causal mechanisms” for the syndrome, which government officials have termed “anomalous health incidents.” These included acoustic signals, chemical and biological agents, ionizing radiation, natural and environmental factors, and radio frequency and other electromagnetic energy.
In the end, the experts determined that “pulsed electromagnetic energy, particularly in the radio-frequency range, plausibly explains the core characteristics” of the health incidents. That finding was not definitive, and “information gaps exist,” the panel wrote in a summary of its findings. But “there are several plausible pathways involving various forms of pulsed electromagnetic energy, each with its own requirements, limitations, and unknowns” that could be making people sick.
Sources of energy exist, the experts wrote, that “could generate the required stimulus” on the human body, and that could be concealed and have “moderate power requirements,” suggesting that the energy could come from a portable device.
Such a device would apparently not be common, but it could be effective. “Using nonstandard antennas and techniques, the signals could be propagated with low loss through air for tens to hundreds of meters, and with some loss, through most building materials,” the summary stated.
Some people who have reported the symptoms said they came on suddenly while they were in offices and hotel rooms. Others have reported the onset while they were outside.
“Ultrasound also plausibly explains the core characteristics,” the experts found, but probably only at close range. The experts’ analysis of ultrasound suggested it might not explain the cases where people fell ill inside a building.
“Ultrasound propagates poorly through air and building materials, restricting its applicability to scenarios in which the source is near the target,” the experts wrote.
State Dept. names new team to oversee ‘Havana Syndrome’ response
Skeptics of a directed-energy attack, perhaps with some form of weapon or surveillance device, have raised the possibility that Havana syndrome victims are actually suffering from some mass delusion or a psychological condition.
But the experts panel cast doubt on that hypothesis.
“Psychosocial factors alone cannot account for the core characteristics, although they may cause some other incidents or contribute to long-term symptoms,” they wrote.
Those core characteristics were helpful in narrowing down the investigation and focusing on aspects of symptoms that “were particularly difficult to explain through other means,” the experts wrote. There were four characteristics, including sound or pressure in the ears; “nearly simultaneous” symptoms such as vertigo, loss of balance and ear pain; “a strong sense of locality or directionality” to those symptoms; and the absence of any known environmental or medical conditions that could have caused them.
The panel acknowledged that some of these symptoms are common in known medical conditions. But the combination of all four “is distinctly unusual and unreported elsewhere in the medical literature, and so far have not been associated with a specific neurological abnormality.”
What’s more, the “location dependence,” or the way symptoms can appear suddenly, and go away quickly, argues for a “stimulus that is spatially and temporally discrete.” All those signs appear to point to some source of energy that is aimed at someone and causes the effects people experienced, the summary shows
An advocacy group of people who say they were the victims of an attack said the new report “reinforces the need for the intelligence community and the broader U.S. government to redouble their efforts to fully understand the causes” of the incidents.
Unanswered questions loom over Biden administration push to strengthen ‘Havana Syndrome’ response
In a joint statement, two top U.S. intelligence officials said the investigation into the cause of the health incidents will continue.
“The U.S. government remains committed to providing access to care for those who need it, and we will continue to share as much information as possible with our workforce and the American public as our efforts continue. Nothing is more important than the well-being and safety of our colleagues,” Avril Haines, the director of national intelligence, and William J. Burns, the director of the CIA, said in a statement.
While investigators have not settled on a cause for the illness, what’s clear is that the overwhelming majority of people who reported symptoms were not the victims of an attack.
Since the first cases were reported at the embassy in Havana in 2016, government investigators have reviewed more than 1,000 cases of anomalous health incidents, a senior CIA official told reporters in January.
The majority of cases could be attributed to a preexisting medical condition or environmental or other factors, the CIA official said. “A few dozen” of those incidents, which the official called “the toughest cases,” could not be explained and would receive further scrutiny.
People familiar with the CIA’s investigation, as well as the work of the expert panel, said that last year, after officials began to encourage anyone suffering from symptoms to report them, a flood of people came forward, most of whom turned out to have some explicable illness or cause behind their symptoms. That kept researchers busy trying to separate wheat from chaff, and ultimately they have zeroed in on that handful of cases that have so far stumped investigators.
The intelligence officials familiar with the panel’s work declined to say how many cases they examined. But the remaining few that have stumped investigators may hold the best chance for ultimately attributing the syndrome to a specific device or country.
—————————————————————————————————————————————————————————
Neuroimaging Findings in US Government Personnel With Possible Exposure to Directional Phenomena in Havana, Cuba
by Ragini Verma 1 2 3 4 5, Randel L Swanson 5 6 7 8, Drew Parker 1 2 4, Abdol Aziz Ould Ismail 1 2 4, Russell T Shinohara 9, Jacob A Alappatt 1 2 4, Jimit Doshi 2 4 10, Christos Davatzikos 2 4 10, Michael Gallaway 11, Diana Duda 12, H Isaac Chen 3 7, Junghoon J Kim 13, Ruben C Gur 14, Ronald L Wolf 2 5, M Sean Grady 3 5, Stephen Hampton 5 6, Ramon Diaz-Arrastia 5 15, Douglas H Smith 3 5
Posted on https://pubmed.ncbi.nlm.nih.gov
on July 23, 2019
Affiliations expand
- PMID: 31334794
- PMCID: PMC6652163
- DOI: 10.1001/jama.2019.9269
Free PMC article
Abstract
Importance: United States government personnel experienced potential exposures to uncharacterized directional phenomena while serving in Havana, Cuba, from late 2016 through May 2018. The underlying neuroanatomical findings have not been described.
Objective: To examine potential differences in brain tissue volume, microstructure, and functional connectivity in government personnel compared with individuals not exposed to directional phenomena.
Design, setting, and participants: Forty government personnel (patients) who were potentially exposed and experienced neurological symptoms underwent evaluation at a US academic medical center from August 21, 2017, to June 8, 2018, including advanced structural and functional magnetic resonance imaging analytics. Findings were compared with imaging findings of 48 demographically similar healthy controls.
Exposures: Potential exposure to uncharacterized directional phenomena of unknown etiology, manifesting as pressure, vibration, or sound.
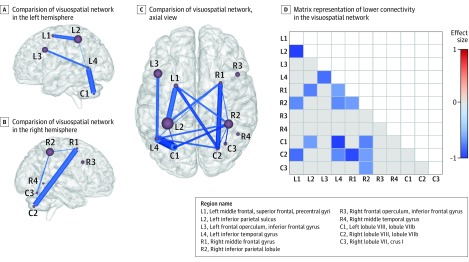
Main outcomes and measures: Potential imaging-based differences between patients and controls with regard to (1) white matter and gray matter total and regional brain volumes, (2) cerebellar tissue microstructure metrics (eg, mean diffusivity), and (3) functional connectivity in the visuospatial, auditory, and executive control subnetworks.
Results: Imaging studies were completed for 40 patients (mean age, 40.4 years; 23 [57.5%] men; imaging performed a median of 188 [range, 4-403] days after initial exposure) and 48 controls (mean age, 37.6 years; 33 [68.8%] men). Mean whole brain white matter volume was significantly smaller in patients compared with controls (patients: 542.22 cm3; controls: 569.61 cm3; difference, -27.39 [95% CI, -37.93 to -16.84] cm3; P < .001), with no significant difference in the whole brain gray matter volume (patients: 698.55 cm3; controls: 691.83 cm3; difference, 6.72 [95% CI, -4.83 to 18.27] cm3; P = .25). Among patients compared with controls, there were significantly greater ventral diencephalon and cerebellar gray matter volumes and significantly smaller frontal, occipital, and parietal lobe white matter volumes; significantly lower mean diffusivity in the inferior vermis of the cerebellum (patients: 7.71 × 10-4 mm2/s; controls: 8.98 × 10-4 mm2/s; difference, -1.27 × 10-4 [95% CI, -1.93 × 10-4 to -6.17 × 10-5] mm2/s; P < .001); and significantly lower mean functional connectivity in the auditory subnetwork (patients: 0.45; controls: 0.61; difference, -0.16 [95% CI, -0.26 to -0.05]; P = .003) and visuospatial subnetwork (patients: 0.30; controls: 0.40; difference, -0.10 [95% CI, -0.16 to -0.04]; P = .002) but not in the executive control subnetwork (patients: 0.24; controls: 0.25; difference: -0.016 [95% CI, -0.04 to 0.01]; P = .23).
Conclusions and relevance: Among US government personnel in Havana, Cuba, with potential exposure to directional phenomena, compared with healthy controls, advanced brain magnetic resonance imaging revealed significant differences in whole brain white matter volume, regional gray and white matter volumes, cerebellar tissue microstructural integrity, and functional connectivity in the auditory and visuospatial subnetworks but not in the executive control subnetwork. The clinical importance of these differences is uncertain and may require further study.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Shinohara reported receipt of personal fees from the American Medical Association and Genentech/Roche, grants and personal fees from the National Institutes of Health, and grants from the Race to Erase MS Foundation and the National Multiple Sclerosis Society. Dr Diaz-Arrastia reported receipt of personal fees, travel support, and stock options from Neural Analytics Inc, grants and nonfinancial support from Brain Box Solutions Inc, and personal fees from BioPharma Partners. No other disclosures were reported.
Figures




Comment in
- Advanced Neuroimaging Findings in US Government Personnel With Possible Directional Phenomenon Exposure in Havana, Cuba.Muth CC, Fontanarosa PB.JAMA. 2019 Jul 23;322(4):348. doi: 10.1001/jama.2019.9746.PMID: 31334774 No abstract available.
- Neuroimaging of US Government Personnel Exposed to Directional Phenomena.Perez DL, Mark VW, Stone J.JAMA. 2019 Dec 10;322(22):2249. doi: 10.1001/jama.2019.16570.PMID: 31821426 No abstract available.
Similar articles
- Neurological Manifestations Among US Government Personnel Reporting Directional Audible and Sensory Phenomena in Havana, Cuba.Swanson RL 2nd, Hampton S, Green-McKenzie J, Diaz-Arrastia R, Grady MS, Verma R, Biester R, Duda D, Wolf RL, Smith DH.JAMA. 2018 Mar 20;319(11):1125-1133. doi: 10.1001/jama.2018.1742.PMID: 29450484 Free PMC article.
- Association of Intensive vs Standard Blood Pressure Control With Cerebral White Matter Lesions.SPRINT MIND Investigators for the SPRINT Research Group, Nasrallah IM, Pajewski NM, Auchus AP, Chelune G, Cheung AK, Cleveland ML, Coker LH, Crowe MG, Cushman WC, Cutler JA, Davatzikos C, Desiderio L, Doshi J, Erus G, Fine LJ, Gaussoin SA, Harris D, Johnson KC, Kimmel PL, Kurella Tamura M, Launer LJ, Lerner AJ, Lewis CE, Martindale-Adams J, Moy CS, Nichols LO, Oparil S, Ogrocki PK, Rahman M, Rapp SR, Reboussin DM, Rocco MV, Sachs BC, Sink KM, Still CH, Supiano MA, Snyder JK, Wadley VG, Walker J, Weiner DE, Whelton PK, Wilson VM, Woolard N, Wright JT Jr, Wright CB, Williamson JD, Bryan RN.JAMA. 2019 Aug 13;322(6):524-534. doi: 10.1001/jama.2019.10551.PMID: 31408137 Free PMC article. Clinical Trial.
- Outcomes at 6 months are related to brain structural and white matter microstructural reorganization in idiopathic tinnitus patients treated with sound therapy.Chen Q, Lv H, Wang Z, Wei X, Zhao P, Yang Z, Gong S, Wang Z.Hum Brain Mapp. 2021 Feb 15;42(3):753-765. doi: 10.1002/hbm.25260. Epub 2020 Oct 24.PMID: 33098363 Free PMC article.
- Diffuse alterations in grey and white matter associated with cognitive impairment in Shwachman-Diamond syndrome: evidence from a multimodal approach.Perobelli S, Alessandrini F, Zoccatelli G, Nicolis E, Beltramello A, Assael BM, Cipolli M.Neuroimage Clin. 2015 Feb 27;7:721-31. doi: 10.1016/j.nicl.2015.02.014. eCollection 2015.PMID: 25844324 Free PMC article.
- Structural neuroimaging of the altered brain stemming from pediatric and adolescent hearing loss-Scientific and clinical challenges.Ratnanather JT.Wiley Interdiscip Rev Syst Biol Med. 2020 Mar;12(2):e1469. doi: 10.1002/wsbm.1469. Epub 2019 Dec 4.PMID: 31802640 Free PMC article. Review.
Cited by 5 articles
- Reply to Orlhac, F.; Buvat, I. Comment on “Ibrahim et al. The Effects of In-Plane Spatial Resolution on CT-Based Radiomic Features’ Stability with and without ComBat Harmonization. Cancers 2021, 13, 1848″.Ibrahim A, Refaee T, Primakov S, Barufaldi B, Acciavatti RJ, Granzier RWY, Hustinx R, Mottaghy FM, Woodruff HC, Wildberger JE, Lambin P, Maidment ADA.Cancers (Basel). 2021 Jun 21;13(12):3080. doi: 10.3390/cancers13123080.PMID: 34205490 Free PMC article.
- Diffusion MRI tractography filtering techniques change the topology of structural connectomes.Frigo M, Deslauriers-Gauthier S, Parker D, Aziz Ould Ismail A, John Kim J, Verma R, Deriche R.J Neural Eng. 2020 Nov 11;17(6):10.1088/1741-2552/abc29b. doi: 10.1088/1741-2552/abc29b.PMID: 33075758 Free PMC article.
- Pulsed Microwave Energy Transduction of Acoustic Phonon Related Brain Injury.Hubler GK, Hoffman SW, Andreadis TD, DePalma RG.Front Neurol. 2020 Aug 4;11:753. doi: 10.3389/fneur.2020.00753. eCollection 2020.PMID: 32849213 Free PMC article.
- Distinctive Convergence Eye Movements in an Acquired Neurosensory Dysfunction.Balaban CD, Szczupak M, Kiderman A, Levin BE, Hoffer ME.Front Neurol. 2020 Jun 16;11:469. doi: 10.3389/fneur.2020.00469. eCollection 2020.PMID: 32655474 Free PMC article.
- Proposal for a new diagnosis for U.S. diplomats in Havana, Cuba, experiencing vestibular and neurological symptoms.Abouzari M, Goshtasbi K, Sarna B, Lin HW, Djalilian HR.Med Hypotheses. 2020 Mar;136:109499. doi: 10.1016/j.mehy.2019.109499. Epub 2019 Nov 18.PMID: 31770686 Free PMC article.
MeSH terms
- Adult
- Brain / anatomy & histology
- Brain / diagnostic imaging
- Brain / pathology*
- Case-Control Studies
- Cuba
- Diffusion Magnetic Resonance Imaging
- Female
- Government Employees*
- Gray Matter / anatomy & histology
- Gray Matter / diagnostic imaging
- Humans
- Magnetic Resonance Imaging
- Male
- Nervous System Diseases / diagnostic imaging*
- Nervous System Diseases / etiology
- Noise / adverse effects
- Organ Size
- Reference Values
- United States
- White Matter / anatomy & histology
- White Matter / diagnostic imaging
Related information
Grant support
LinkOut – more resources
- Full Text Sources
- Medical